Occupational Therapy interventions to address axillary web syndrome: A debilitating side effect of breast cancer treatment
 Occupational Therapy interventions to address axillary web syndrome: A debilitating side effect of breast cancer treatment
Occupational Therapy interventions to address axillary web syndrome: A debilitating side effect of breast cancer treatment
Brittany Hypes, OTD, OTR/L, CSRS, C-MLD, Kaye Rubio, Ph.D., MHS, OTR/L, CLT-LANA, & Kristin Domville, OTD, MOT, OTR/L
Snip it: Read about axillary webbing or cording in this case report and the occupational therapy treatment that was provided to address limited shoulder movement.
Abstract: Axillary web syndrome (AWS) is a complication of breast cancer (breast cancer) surgery, with an incidence of 6% to 86%. It presents as tight, painful cords in the axilla, limiting shoulder range of motion and performance of daily activities. This presentation will help occupational therapists recognize AWS and suggest treatments to address AWS. It is a case study of two breast cancer survivors referred to outpatient an occupational therapy clinic where a microcurrent device was used to address the limitations related to AWS.
Introduction
The incidence of breast cancer has increased by 0.5% each year, with 297,000 new cases expected in 2023 (breastcancer.org, 2023). Axillary web syndrome (AWS) is a complication of breast cancer surgery, with an incidence of 6% to 86% (Tay et al., 2021). AWS is caused by lymphovenous damage that results in sclerosed veins and lymphatics, fibrosis, and lymphatic stasis. It can occur following surgical procedures such as mastectomy, node-positive breast cancer, lumpectomy, and lymph node removal (Roman et al., 2022; Tay et al., 2021; Smith, 2019; Koehler et al., 2018). As a result, it can reduce a patient’s range of motion including shoulder flexion and shoulder abduction as well as pain and discomfort with movement. AWS presents as taut, tight cords in the axilla, and medial upper arm, extending to the forearm or chest wall. It limits shoulder range of motion (ROM) due to tightness and pain limiting the person's ability to perform daily activities.
Literature has identified the benefits of therapy interventions such as scar management, lymphatic drainage, patient education, supervised and in-home exercise programs. Occupational therapy plays a vital role in helping breast cancer survivors face the long-term effects of treatment (Shin et al., 2021). This case report involves two breast cancer survivors who developed AWS. The occupational therapist used MPS to address the tight cords in the axilla.
About Microcurrent Point Stimulation
The Dolphin Microcurrent Point Stimulation device provides reduction of soft tissue pain throughout any area of the body and applies DC microcurrent impulses that can help relax the central nervous system and therefore reduce pain and stress. The use of the Microcurrent Point Stimulation (MPS) device helps to break down the cording and scar tissue at a cellular level and helps to achieve adequate range of motion. MPS devices can incorporate myofascial scar release techniques to improve pain levels using the visual analog scale up to 59% after the initial treatment session with pain associated with the AWS (Armstrong et al., 2017).
Method
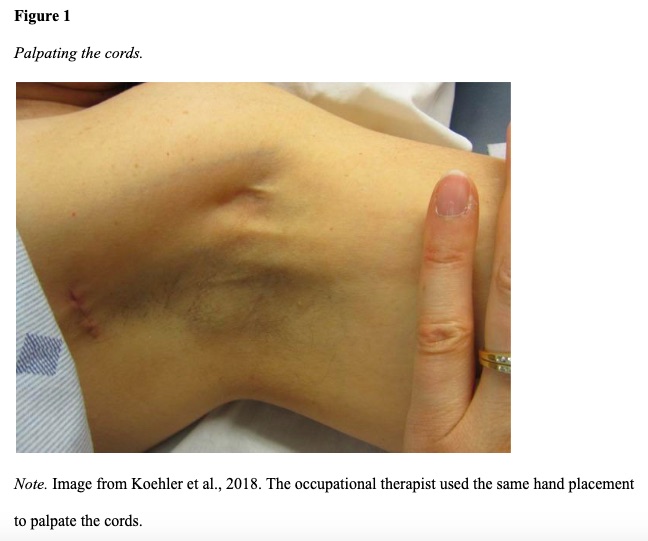
The two clients were referred to outpatient OT to address complications following breast cancer surgery and treatment. They reported inability to return to work and difficulty performing vital occupations such as child care and home management, feelings of uncertainty regarding the cause of pain, loss of ROM, and lack of knowledge regarding pain after breast cancer surgery. AWS was identified by placing the affected shoulder in abduction while applying tension on the skin (see Figure 1).
Initial evaluation
Case 1 is a 58-year-old client who underwent mastectomy with axillary lymph node dissection. The client presented with 3/10 pain in the right shoulder. Active shoulder flexion ROM was 115 degrees and abduction was 100 degrees. Case 2 is a 55-year-old client who underwent bilateral mastectomy and axillary lymph node dissection. The client presented with 3/10 pain with shoulder movement. Active shoulder flexion ROM was 135 flexion and 125 degrees of abduction. Both clients reported pain due to a “pulling” sensation in the axilla that feels tight when they move the shoulder.
 Occupational therapy intervention
Occupational therapy intervention
OT intervention included patient education on pain syndromes related to breast cancer, a home program for manual lymph drainage and stretching, activity modifications, supervised stretching, and MPS. The MPS device was used to soften the axillary web at a cellular level to reduce pain and increase ROM. The MPS protocol that was implemented began with scar release therapy (SRT). This technique utilized two MPS devices on (-) and (+/-) polarity starting at the breast scar and treated in a horizontal motion 3x leaving each point on for about 15-20 seconds (see Figure 2). Afterward, the occupational therapist palpated the area to identify the cords along the arm. MPS is then applied in a horizontal motion on each area for 20-30 seconds 3-4x depending on the severity of the cording. The MPS protocol is followed by gentle myofascial release and stretching of the affected shoulder and elbow.
Results
Case 1 reported 0/10 pain with Active shoulder flexion of 140 degrees and abduction of 125 degrees after 4 months of OT, 2x a week. Case 2 reported 0/10 pain with Active shoulder flexion of 175 degrees and abduction of 180 degrees after 4 months of OT, 2x a week. The two clients reported significant pain reduction, increased shoulder ROM, and improved engagement in valued roles
Conclusion
Based on various cases treated by the occupational therapist since offering MPS at the outpatient clinic, it has been shown that pain levels have been reduced almost to 0/10 pain as well as maximizing functional use of the shoulders which results in the patient's being able to engage in their ADLs and as well as work-related activities. This case report presented information regarding AWS and suggested treatment activities to enable breast cancer survivors to regain participation in meaningful roles.
References
Armstrong, K., Gokal, R., Durant, J., Todorsky, W., & Miller, L. (2017). The successful treatment of chronic pain using microcurrent point stimulation applied to scars. International Journal of Complementary and Alternative Medicine, 10(3), 1-4. doi: 10.15406/ijcam.2017.10.00333
Breastcancer.org. (2023). Breast cancer facts and statistics. https://www.breastcancer.org/facts-statistics
Koehler, L. A., Hunter, D. W., Blaes, A. H., & Haddad, T. C. (2018). Function, shoulder motion, pain, and lymphedema in breast cancer with and without axillary web syndrome: An 18-month follow-up. Physical Therapy & Rehabilitation Journal, 98(6), 518–527. https://doi.org/10.1093/ptj/pzy010
Roman, M. M., Barbieux, R., Eddy, C., Karler, C., Veys, I., Zeltzer, A., Adriaenssens, N., Leduc, O., & Bourgeois, P. (2022). Lymphoscintigraphic investigations for axillary web syndromes. Lymphatic Research and Biology, 20(4), 417–424. https://doi.org/10.1089/lrb.2021.0015
Shin, C., Amanat, Y., & Morikawa, S. (2021). Occupational therapy’s role across the continuum of care for patients with breast cancer. SIS Quarterly Practice Connections, 6(3), 28–30.
Smith, C. (2019). Cording: A treatable complication of breast cancer surgery. The British Journal of General Practice, 69(685), 395. https://doi.org/10.3399/bjgp19X704825
Tay, M. R. J., Wong, C. J., & Aw, H. Z. (2021). Prevalence and associations of axillary web syndrome in Asian women after breast cancer surgery undergoing a community-based cancer rehabilitation program. BMC Cancer, 21(1), 1019. https://doi.org/10.1186/s12885-021-08762-z